
Abstract
We report a case of cholesteatoma associated with unilateral congenital aural atresia (CAA) and microtia, resulting in extracranial complication. A 13-year-old girl presented with right ear purulent discharge from pre and post auricular area with mastoid tenderness. On clinical examination, she had right grade II microtia with pre-auricular skin tag and healed scar tissue in periauricular region. On High Resolution Computerized Tomography (HRCT) scan of temporal bones, there was CAA of right ear with extensive cholesteatoma in middle ear cleft. The cholesteatoma was subsequently removed by radical mastoidectomy with uneventful post-operative period. Cholesteatoma associated with CAA may remain undiagnosed in early childhood resulting in life threatening temporal and intracranial complications.
Author Contributions
Academic Editor: Cuneyt Kucur, Dumlupinar University
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Rahul Kumar Singh, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Congenital aural atresia (CAA) refers to a spectrum of ear deformities present at birth that involves some degree of failure of the development of the external auditory canal (EAC). The incidence of congenital aural atresia is 1 in 10,000 to 1 in 20,000 live births1. Microtia has an incidence of 1 in 7000 to 8000 births in the general population 2, 3. Males are affected more commonly, and the reported ratio of right-to-left-to-bilateral is approximately 5:3:1 with bilateral deformity occurring in only 10% of patients4, 5, 6, 7.
Case Report
A 13 year old girl presented in ENT outpatient department with complains of recurrent right ear purulent discharge from pre and post auricular area for last 5 years. She had a history of incision and drainage in right post auricular area six months prior for similar complain. On local examination, there was right Grade II8microtia with atretic External Auditory Canal (EAC) and pre-auricular skin tag (Figure 1). A small fistulous opening was also seen in right cavum conchae region. Left ear examination was normal with intact tympanic membrane. Tuning fork tests using 256 and 512 Hz tuning forks showed moderate to severe conductive hearing loss in right ear with Rinne’s test positive in left ear. HRCT scan of temporal bones showed membranous atresia of right EAC with grade II microtia. Soft tissue density was seen filling the EAC and the entire middle ear cavity (Figure 2A). A CT based fistulogram done four months before our consultation identified multiple fistulous tracts situated in post auricular region and anterior to stylomastoid foramen in inframastoid region. These fistulous tracts were communicating through middle ear cavity (Figure 2B). There was associated erosion of posteroinferior and anteroinferior wall of EAC. Ossicles were dysplastic or eroded. Inner ear structures were normal. Patient underwent right radical mastoidectomy with wide conchal meatoplasty under general anaesthesia. Intraoperatively, there was right EAC membranous atresia with fistulous opening in cavum conchae. Cholesteatoma sac was seen filling the mastoid antrum area extending into middle ear cavity and EAC with erosion of posterior canal wall. Except remnant of malleus head which was fixed to epitympanic wall, no other ossicle was found. Oval window area showed bony depression without any overlying stapes footplate (Figure 3). Lateral semicircular canal bulge, facial nerve canal and chorda tympani were found at their usual locations (Figure 4). Obliteration of mastoid cavity posterior to vertical segment of bony facial canal was done using pedicled temporalis muscle flap to reduce the size of postoperative cavity. Middle ear cavity was covered with temporalis fascia graft.
Figure 1.showing Right grade II microtia
Figure 2.(A-B) HRCT imaging. (A) Right canal atresia with soft tissue density behind it (B) CT sino-gram showing multiple (arrow marked) sinuses communicating to right middle ear cavity.
Figure 3.Arrow pointing towards oval window area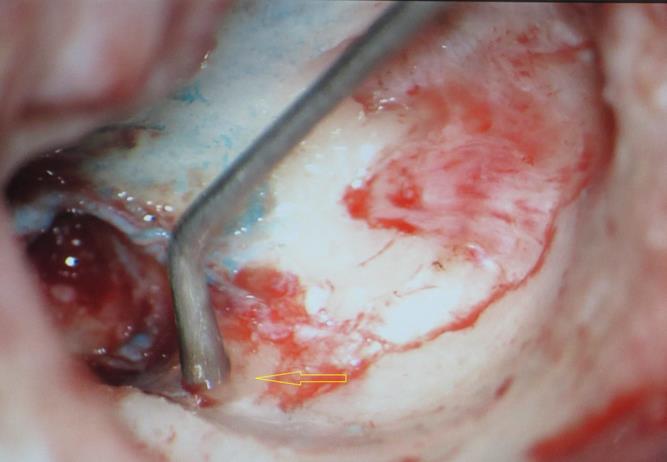
Figure 4.Arrow pointing to exposed facial nerve (vertical segment)
Discussion
The dominating feature of congenital aural atresia is absence of the external auditory canal. It is commonly unilateral, more frequently involving the right ear9. While associated abnormalities of the auricle are common, the inner ear development of these patients is most often normal. Similar findings were seen in our case with disease limited to right external and middle ear.
Cholesteatoma formation in atretic ears have two different patterns, one with ear canal of diameter 4 mm or smaller in which cholesteatoma formation is attributed to invagination of small pouch lined with ectoderm within the canal itself. Other mode is the development of the cholesteatoma medial to the atretic plate or inside the tympanic cavity. The occurrence of latter type is explained by the trapping of the epidermoid elements during the embryological arrest of the EAC formation so as to form a nidus for the cholesteatoma behind the atresia plate10. This theory is known as “embryological rest” theory and was credited as one of the possible mechanisms of congenital cholesteatoma development 11.
Zalzal et al (1987) reported a case of a two year old boy with congenital aural atresia complicated by acute mastoiditis and lateral sinus thrombosis due to concurrent cholesteatoma 12. Nishimura et al (1985) reported another cholesteatoma case with aural atresia, arising behind the atresia plate that also caused mastoditis and subperiostal abcess 13.Cole and Jahrsdorfer (1990) 14reported the largest series of cholesteatoma and aural stenosis association. They found 48% of their EAC stenosis patients (with the ear canal smaller than 4 mm diameter) developing cholesteatoma and none of them were under the age of three. More strikingly, they found cholesteatomous developments in 91 % (10 out of 11) patients with ear canal diameters of 2 mm or less. Hidden large cholesteatoma has been missed out in our patient due to inability to examine an atretic ear canal. When cholesteatoma is located behind atretic or stenotic canal segment, the risk of extra-temporal complications such as mastoiditis, cutaneous fistula and intracranial extensions are greater due to the hindrance of growth and drainage towards the nonexistent or severely narrowed EAC 15.Cutaneous fistulae were seen in post auricular, inframastoid and cavum conchae region in our patient along with history of associated mastoid tenderness. These fistulae were also identified in CT based fistulogram.
Given the severity and frequency of complications resulting from cholesteatoma, mastoidectomy is necessary to determine the underlying pathology and to control the disease process 16, as was done in our patient.
In 2006, Caughey et al 17 reported a case of CAA with congenital cholesteatoma medial to the atretic plate, with no ossicular erosion. The authors had removed the malleus-incus complex to facilitate complete removal of cholesteatoma and the conductive hearing mechanism was reconstructed using partial ossicular replacement prosthesis. However, our case showed no malleus-incus complex (ossicular erosion due to cholesteatoma or total ossicular dysplasia) without any identifiable oval or round window. Removal of cholesteatoma with clearance of pathological mucosa and a wide mastoid cavity was the aim before and during surgery.
Conclusion
All patients presenting with aural atresia and stenosis should be evaluated thoroughly due to their propensity to develop cholesteatoma. Radiological evaluation in the form of HRCT scan of temporal bones should always be done in these patients during their initial presentation itself and surgery planned accordingly. This will help in preventing late and life threatening intracranial complications as a result of undetected cholesteatoma associated with CAA. The aim of surgery should be to remove the disease and reconstruct a patent, infection-free external auditory canal along with restoration of functional hearing if possible.
References
- 1.Rosen E J, Gadre A K, Quinn F B, Ryan M W.. 2003Jan; Congenital Aural Atresia. UTMB, Department of Otolaryngology & Lambert PR, Dodson EE. Congenital Malformations of the External Auditory Canal. Otolaryngologic clinics of North America1996Oct; 29(5), 741-760.
- 2.Aguilar E F. (2001) Auricular reconstruction in congenital anomalies of the ear Facial Plast Surg Clin North Am. 9, 159-169.
- 3.Romo T. (2000) Fozo MS, Sclafani AP Microtia reconstruction using a porous polyethylene framework. Facial Plast Surg. 16, 15-22.
- 4.Shaw G M, Carmichael S L, Kaidarova Z, Harris J A. (2004) Epidemiologic characteristics of anotia and microtia in California,1989-1997. Birth Defects Res A Clin Mol Teratol2004;. 70, 472-5.
- 5.Harris J, Kallen B, Robert E. (1996) The epidemiology of anotia and microtia. , J Med Genet 33, 809-13.
- 6.Okajima H, Takeichi Y, Umeda K, Baba S. (1996) Clinical analysis of 592 patients with microtia. Acta Otolaryngol Suppl. 52, 18-24.
- 7.Melnick M, Myranthopoulus N C. (1979) External ear malformations: epidemiology, genetics and natural history. , In: Birth Defects. Vol 15.
- 8.Ogino Y, Nishimura Y, Horii M. (1976) Congenital microtia – multidirectional tomographic and remnant auricular forms. Pract Otol. 69, 792-801.
- 9.Doyle K J, Ray R M. (2003) The otolaryngologist role in management of hearing loss in infancy and childhood.Ment Retard Dev Disabil Res Rev. 9, 94-102.
- 10.Miyamoto R T, Fairchild T H, Daugherty H S. (1984) Primary cholesteatoma in the congenitally atretic ear.Am J Otol. 5, 283-285.
- 11.Semaan M T, Megerian C A. (2006) The pathophysiology of cholesteatoma.Otolaryngol Clin North Am. 39, 1143-1159.
- 12.Zalzal G Y. (1987) Acute mastoditis complicated by sigmoid sinus thrombosis in congenital aural atresia. , Int J Ped Otorhinolaryngol 14, 31-39.
- 13.Nishimura Y, Kumoi T, Sano S.Cholesteatoma auris congenita arising from microtia. Ann Plast Surg1985;. 14, 296-300.
- 14.Cole R R, Jahrsdoefer R A. (1990) The risk of cholesteatoma in a case of congenital aural atresia. , Laryngoscope; 100, 576-8.
- 15.Yildirim Nadir, Sahan Murat.Abdullah Akkaya: Primary Cholesteatoma within the Stenotic Ear Canal: Report of two Cases, one with Extra-Temporal Complications. , Int. Adv. Otol. 2009; 5 :( 2, 281-285.
Cited by (2)
- 1.Fourla Natalia V, Chrysikos Dimosthenis T, Makrypidis Konstantinos T, Memtsas Zacharias A, Protogerou Vasileios D, et al, 2022, Unilateral aural atresia: a case report, Journal of Surgical Case Reports, 2022(2), 10.1093/jscr/rjac037
- 2.Thangavel Saranya, Penubarthi Lokesh Kumar, Alexander Arun, Saxena Sunil Kumar, 2021, Surgical corridors for congenital aural atresia with otogenic cerebellar abscess and lateral sinus thrombosis, BMJ Case Reports, 14(5), e239403, 10.1136/bcr-2020-239403