
Implementing Evidence-Based Occupational Therapy for Multiple Sclerosis Rehabilitation: Exploring Knowledge on Barriers, Facilitators and Strategies
- Open Access
- Peer Reviewed
- Similarity Checked
- CC BY 4.0
Abstract
Background
A persistent gap remains between evidence-based health care and its application in routine practice. This challenge is particularly prominent in allied health professions like occupational therapy (OT), where interventions are complex, individualized and centred on patients' daily functioning.
Objective
To identify barriers, facilitators, and implementation strategies for integrating evidence-based OT interventions in multiple sclerosis (MS) rehabilitation.
Methods
A mapping review was conducted using searches in five databases. Eligible studies included adults with MS, examined OT interventions, and reported on factors influencing implementation. Data were extracted and categorized using Grol’s framework for barriers/facilitators and Mazza’s taxonomy for implementation strategies.
Results
Fifteen studies met inclusion criteria. Barriers and facilitators were identified at multiple levels of Grol’s framework: 1-Innovation-level: accessibility, feasibility, and perceived attractiveness supported implementation, particularly when interventions incorporated holistic approaches, gamification, or printed manuals. 2-Professional-level: therapists’ competencies and alignment between interventions and patients’ priorities. 3-Patient-related: facilitators included motivation, readiness to change, and peer support, whereas fatigue, pain, and cognitive challenges served as barriers. 4-Social and organizational: effective teamwork, resource availability, and flexible scheduling facilitated successful adoption. 5-Economic or political: no studies.
Implementation strategies focused on using manuals, patient empowerment, gamification, and organizational supports. No financial or structural policy-level strategies were identified.
Conclusion
Successful implementation of evidence-based OT for MS requires multifaceted, context-sensitive strategies addressing innovation, professional, patient, and organizational determinants. Practical approaches enhance uptake, while substantial gaps persist at economic and policy levels. Strengthening these areas may improve longterm integration and sustainability of evidence-based OT in MS rehabilitation.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Leen De Coninck, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Daphne Kos, KU Leuven, Department of Rehabilitation Sciences, Tervuursevest, 101, PO box 1501, 3001 Leuven, Belgium, Rehabilitation Research, National Multiple Sclerosis, Center, Melsbroek, Belgium —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Healthcare systems are increasingly accountable for delivering care that is effective, safe, and cost-efficient 1. However, despite substantial advances in research, a persistent gap remains between the generation of evidence and its uptake in clinical practice. The underutilization of research findings by healthcare professionals is a prevalent challenge across the healthcare sector 2. Understanding the barriers and facilitators that influence the adoption of evidence-based interventions is therefore critical to ensuring that innovations are implemented as intended and achieve their desired impact.
Implementation science focuses on optimizing the integration of evidence-based innovations into routine practice and examines how implementation strategies can support this process 3. A range of implementation theories, models and frameworks have been developed for this purpose, including the Knowledge to Action Model 4. These tools can systematically identify potential barriers and facilitators, thereby inform the selection and tailor of implementation strategies, guiding necessary adaptations, and clarification of outcomes. Applying an implementation model such as the 5-Step Approach of Peters 5, has shown to be successful in addressing barriers and facilitating changes in practice 6. This approach typically involves several stages: identification (analyzing knowledge gaps and selecting the novel intervention), context analysis (understanding barriers and facilitators), developing an action plan (linking and tailoring action to identified barriers and facilitators, selecting quality indicators, and initiating implementation), evaluation (assessing progress and adjusting as needed) and striving for sustainability planning (embedding in routine care) 5.
Implementing evidence-based interventions in occupational therapy (OT) is essential to support people with multiple sclerosis (PwMS) in managing symptoms such as fatigue, muscle weakness, impaired coordination, and cognitive problems. OT is a client-centered profession that promotes health and wellbeing through engagement in everyday activities. Its core aim is to enable participation in meaningful activities by enhancing individuals’ ability to manage symptoms and perform daily activities, often through targeted activity or environmental modifications 7.
Recent evidence synthesized in a Cochrane review, confirm that OT interventions can improve daily functioning and aspects of quality of life of people with MS, while also emphasizing the need for improved implementation to ensure these benefits are realized in routine care 8.
Occupational therapy practice is complex, involving diverse service users and interventions. To support the adoption of evidence-based practices within this complexity, several theoretical frameworks and models have been developed to help identify barriers and facilitators and to guide the selection of appropriate implementation strategies 9, 10, 11. These frameworks provide structured approaches to designing implementation plans tailored to the specific context of OT practice.
Commonly used change interventions include educational strategies, audit and feedback, reminders, task substitution, multiprofessional collaboration, quality management initiatives, financial incentives, patient-mediated interventions, and combinations of these approaches 10. The modified Mazza framework 11 categorizes implementation actions into five groups: professional-level, patient/consumer-level, financial (for both providers and patients), organizational (for both providers and patients), and structural changes.
By systematically identifying barriers and facilitators to implementation, OT can progress toward more consistent, effective and evidence-based service delivery. Strengthening implementation efforts ultimately has the potential to improve the quality, efficiency, and outcomes of OT services, thereby enhancing the wellbeing and independence of PwMS. This mapping review synthesizes current evidence on the implementation of OT interventions for PwMS.
The objective of this study is to identify barriers, facilitators and implementation strategies relevant to occupational therapists when integrating evidence-based occupational therapy interventions for adults with multiple sclerosis in physical rehabilitation settings.
Methods
Study design
A mapping literature review of international peer-reviewed health research articles was conducted following established mapping review guidelines 12. Mapping reviews aim to outline the current state of evidence of a specific topic and incorporate a framework that guides data extraction, making this approach suitable for our research objective 12, 13.
An international, multidisciplinary research team (Belgium, Ireland, United Kingdom and The Netherlands) consisting of a person with lived experience, five occupational therapists (three of whom were both researchers and practitioners), one nurse, one physical rehabilitation scientist, one senior student in medicine, one methodologist and one MS specialist physiotherapist prepared, monitored, and discussed the outcomes of the review steps. Team members periodically reviewed draft versions individually and met monthly to discuss and revise the manuscript at each stage of the review process, including defining the scope, in- and exclusion criteria, database selection, review of the study selection and analysis procedures, data synthesis and successive draft versions of the article.
Search strategy
Five databases were searched by one researcher (LD): Medline via PubMed, EMBASE via Elsevier, CINAHL via EBSCO, ERIC via EBSCO, and OTDbase. Medline and EMBASE were the primary databases. Medline provides an overview of biomedical and life sciences literature. EMBASE is a major biomedical and pharmacological database, offering comprehensive coverage of clinical medicine, public health, environmental health, rehabilitation, and physical therapy. To ensure coverage of allied health, education, and occupational therapy-specific journals, these two databases were supplemented with CINAHL (allied health literature), ERIC (education research and information) and OTDbase (occupational therapy journals).
A structured search strategy was developed and adapted to each database. Given the large number of articles, a specific search for the databases Medline and EMBASE was established. For CINAHL and Eric, the terms ‘Occupational Therapy’ and ‘Multiple Sclerosis’ were combined. In the OTDbase, the single search term ‘Multiple Sclerosis’ was used due to the nature of this profession-specific database. The search strings are reported in the supplementary data (See Supplement 1). Limits for all searches were research studies written in English or French, published between January 2014 and end of April 2025.
Data selection and extraction
Two researchers (LD, JS) independently performed study selection. Conflicts were solved by discussion.
Eligible for inclusion was any study or review that reported on (1) adults with MS, (2) OT intervention as a monodisciplinary intervention, or as part of a multidisciplinary intervention, interprofessional approach, or OT-like interventions such as improving daily functioning performed by another health professional, and (3) barriers and facilitators of implementing an evidence-based intervention, or actions to turn barriers into facilitators/neutral or to promote implementation of an intervention. Excluded were expert opinions, editorials, conference proceedings, and references on which no full text was available.
One researcher who conducted the search performed the data extraction (LD). The following data were extracted: research design, profession and/ or setting, population, intervention, barriers or facilitators, and implementation strategies.
Data analysis
One researcher (LD) listed the reported barriers and facilitators and subsequently structured them in a literature matrix based on the different levels described in Grol’s framework 14: nature of the innovation; characteristics of the professionals and patients involved; and the social, organisational, economic and political context. This matrix of extracted data was presented to the international team for verification. Based on their feedback, selected data extractions were expanded to ensure clarity and comprehensibility. The analysis of included articles was guided by operationalization of Grol's framework, with facilitators and barriers to evidence implementation specifically mapped in relation to the target population and setting of interest.
The implementation actions were mapped into a literature matrix conforming to the taxonomy of Mazza 11. The taxonomy of Mazza categorizes the actions of implementation interventions into five groups: professional, consumer, financial, organizational and structural changes. This structured approach ensured a comprehensive and systematic analysis of both the factors influencing implementation and the strategies used to address them.
Results
The search identified 337 unique articles (see Figure 1). Of these, 22 underwent full-text review, and 15 studies were included. (See Supplement 2)
Figure 1. PRISMA (2020) flow diagram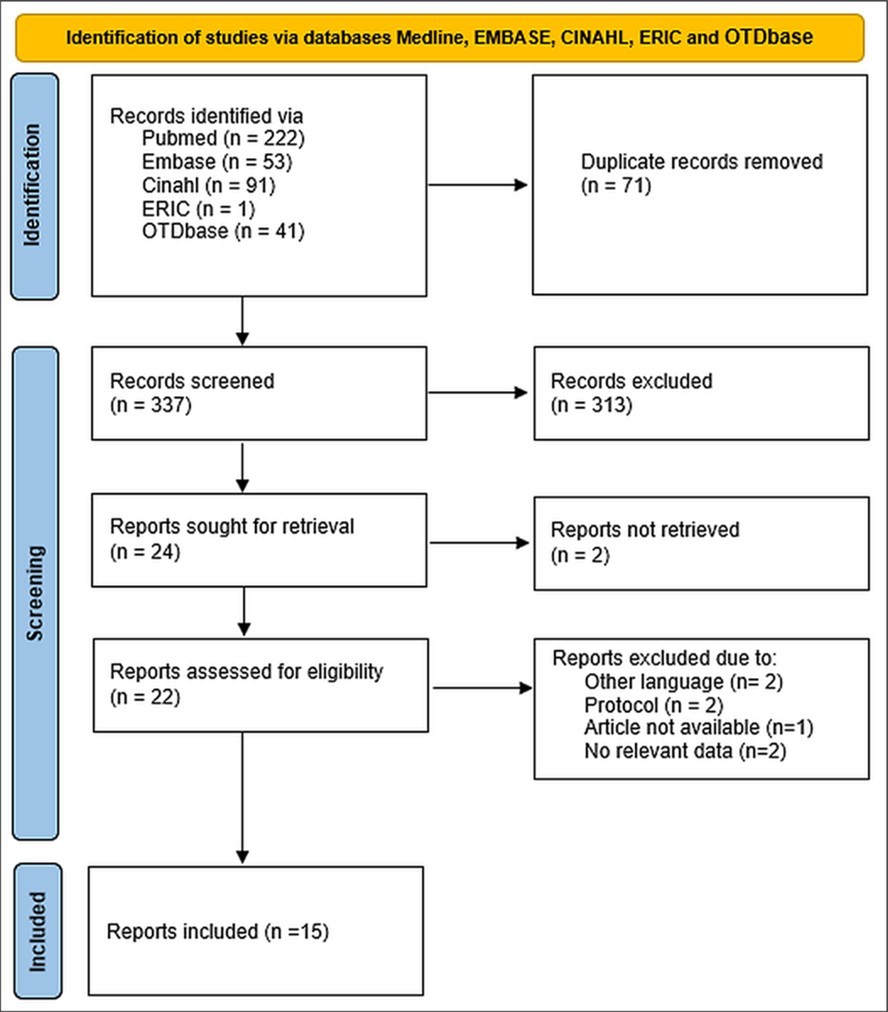
Download figure
The included studies were feasibility studies (n=5), qualitative studies (n=4), a mixed method study (n=1), a descriptive study (n=1), a systematic review (n=1), an RCT (n=1) and a secondary analysis of RCT (n=1), and a quasi-experimental study (n=1). Across these studies, a range of facilitators and barriers were identified (See Table 1) as well as implementation actions (See Supplement 2).
Table 1. Facilitators and barriers influencing adoption of occupational therapy interventions for persons with multiple sclerosis, mapped to Grol’s framework 14.| Grol’s level | Key determinants | Description/examples (illustrative references) |
|---|---|---|
| Innovation | Accessibility and attractiveness | Initial experience with the intervention, perceived accessibility and appeal influenced uptake 15. |
| Feasibility and adaptability | Ability to tailor intervention to the person’s needs, including culturally specific terminology 16, 17, technological components 18, personal preferences and needs 19, pacing 20, experiencing meaningfulness 20, and future adaptation 21. | |
| Holistic integration | Embedding interventions within a holistic approach is appreciated by PwMS and facilitates implementation 21. | |
| Engagement and novelty | Gamification, novelty 22, 15, or a competitive element 15 makes the intervention more attractive, increasing enjoyment and uptake | |
| Perceived effectiveness | Observable functional improvements enhanced adoption 15. | |
| Educational and experiential components | Combining didactic education and experiential learning promoted uptake of an innovative intervention 16. | |
| Tangible materials | Printed manuals aided note-taking, preparation, and post-intervention review 16. | |
| Individual professional | Intervention–problem fit | Alignment between intervention and patient’s problems fostered credibility and uptake 21. |
| Holistic and graded delivery | Grading activities within a holistic person–occupation–environment framework facilitated adoption 18. | |
| Coaching approach | Use of coaching principles enhanced deployment 23. | |
| Professional competencies | Competences of the OT affect the adoption of innovative interventions 24. Skills include emotional intelligence, active listening and group leadership 20, understanding patient needs 18, and time management 17. | |
| Patient | Goal alignment and meaningfulness | Adherence was influenced by alignment with individual goals and meaningfulness of activities 25, 23. |
| Personal, emotional, physical, cognitive factors | Motivation and interest 20, 26, temperament 26, readiness to change 15, and personality traits (resilience, positive mindset) 26. MS-related factors (fatigue, pain, sleep, cognitive challenges) affected uptake 26. | |
| Pace adjustment | Tailoring intervention tempo to the individual facilitated adoption 20. | |
| Peer support and affirmation | Social recognition and peer contact promoted engagement 16, 17, 18, 20, 27, 28. | |
| Social context | Healthcare team support | Support from the healthcare team facilitated implementation 26. |
| Organizational context | Time, resources, and logistics | Availability of time, staff, dedicated resources and equipment 17, 28, flexibility in support hours 24, and scheduling facilitated uptake 28. |
| Economic and political context | — | No determinants were identified in the reviewed literature. |
Facilitators and barriers
Facilitators and barriers to implementing evidence-based occupational therapy interventions for PwMS were identified at multiple levels. An overview of these identified facilitators and barriers is provided in a literature matrix that is included in Table 1.
Innovative level
At the innovation level, the literature highlighted that determinants of deployment include accessibility, attractiveness, feasibility, considering a holistic approach, gaming and competitive components, perceived effectiveness, educational and physical components and the availability of a –tangible, printed manual.
Professional level
Professional-level facilitators included a good fit between the intervention and the patient’s problems, the ability to grade activities within a holistic approach (including the person, the occupation and the environment), and the use of coaching principles. Professional competencies such as emotional intelligence, active listening, leadership, understanding patient needs, and time management, were also facilitators.
Patient level
At patient level, adherence is promoted by goal alignment and meaningfulness (alignment with individual goals and meaningfulness of activities), personal, emotional, physical, and cognitive factors (motivation and interest, temperament, readiness to change, personality traits such as resilience and positive mindset, and MS-related factors like fatigue, pain, sleep, and cognitive challenges, pace adjustment (tailoring intervention tempo to the individual), and peer support and affirmation (social recognition and peer contact).
Social context
A key social context facilitator was support from the healthcare team.
Organizational context
Organizational facilitators included sufficient time, resources, flexible support, and effective scheduling.
Economic and political context
No determinants were identified at the economic or political level.
Implementation actions
The literature review identified implementation strategies across three levels: professional, consumer, and organizational.
Professional level
Identified professional-level implementation strategies included the use of tools such as the Medical Research Council (MRC) Guidelines for complex interventions 21, the provision of intervention manuals 16, 21, 28 and the visualization of knowledge to support intervention delivery 16. Additional strategies involved providing links to partner organizations’ websites to facilitate access to resources 16. Conscious collaboration between therapists and persons with MS and the systematic collection of participant feedback throughout all stages of the intervention 25 were also reported as effective implementation strategies.
Consumer focused level
A consumer-focused action emphasizes the empowerment of the patient. Empowerment aimed at fostering independence and self-management was promoted by addressing determinants such as knowledge, risk perception, outcome expectation, self-efficacy, coping strategies, action control, and outcome experience 28. Incorporating the principles of gamification 15, 22 and continually adjustment and tailoring the intervention to individual's needs 18, 23, 25 were perceived as meaningful implementation strategies. Adjusting and tailoring also included grading both the technology and therapeutic goals.
Organizational level
At the organizational level, technical organizational actions included providing a formal contract to enhance role clarity and reduce concerns among stakeholders 15. Active leadership engagement is also seen as a supportive organizational implementation strategy 21.
No implementation strategies regarding financial incentives, or regulatory or structural changes were identified in the reviewed literature.
An overview of the identified implementation strategies is provided in a literature matrix included in the supplementary material (See Supplement 3).
Discussion
This mapping review highlights the inherently multi-level nature of implementing evidence-based occupational therapy (OT) interventions for people with multiple sclerosis (PwMS). Using Grol’s framework, the findings indicate that implementation is shaped by interacting determinants rather than isolated factors, underscoring the need for comprehensive, theory-informed implementation planning.
Successful implementation of evidence-based OT for MS requires multifaceted, context-sensitive strategies. Our review demonstrates that successful implementation of OT interventions for PwMS relies on strategies operating across multiple levels of Mazza’s taxonomy 11. At the professional level, structured guidance, accessible resources, and collaborative therapeutic relationships support consistent and high-quality intervention delivery. Consumer-focused strategies underscore the importance of empowering PwMS through tailored approaches that enhance self-management, motivation, and engagement 29, 30. Organizational strategies, though less frequently reported, highlight the value of clear role delineation and active leadership in creating an environment conducive to implementation. The absence of identified economic–political determinants likely reflects a gap in the literature, indicating an important direction for future research.
Altogether, our findings emphasize the need for multilevel, coordinated implementation efforts and point to opportunities for future work to address underexplored systemic determinants that may further strengthen the adoption and sustainability of OT interventions for this population.
Actions to adopt evidence-based interventions often occur late in the research process, after study results have been published. However, evidence shows that strong early-stage implementation planning substantially increased the likelihood of successful uptake and delivery of interventions 31. Over the past decade, several initiatives have sought to improve the reporting of interventions. For example, the use of the TIDieR (Template for Intervention Description and Replication) checklist is a valuable tool to inform both researchers and clinicians about intervention delivery 32. Although TIDieR represents an important advance, it may not completely convey the complexity of rehabilitation (including OT) interventions. In response, the Cochrane group recently developed the Guideline for Intervention Description in Rehabilitation (GUIDE-Rehab) 5, which aims to better reflect the multi-faceted nature of rehabilitation practice. These initiatives may support the evidence of adoption by occupational therapists working in MS rehabilitation. However, language barriers may hinder the use of these resources, most often written in English. Therefore, locally delivered educational initiatives led by professional organizations are needed to facilitate optimal implementation for example by developing and disseminating translated summaries or practical guides in the local language, and by offering workshops or webinars tailored to the national context. Regulatory bodies may also support this process, by establishing standards, rules, and guidelines that define how interventions should be implemented - although evidence supporting their role remains lacking.
This mapping review is characterized by several strengths, like its systematic and transparent search strategy, which was developed and executed across five major databases spanning biomedical, allied health, educational, and OT specific sources. By clearly documenting the databases and search parameters, the review aligns with recommendations from the PRISMA framework 33, thereby enhancing the reproducibility and credibility of the process. The breadth of databases also ensured that the review captured a wide range of perspectives relevant to OT and multiple sclerosis, reducing the risk of missing disciplinespecific literature.
Furthermore, the use of two wellestablished theoretical frameworks—Grol’s model of barriers and facilitators 14 and Mazza’s taxonomy of implementation strategies 11— guided the data extraction and synthesis. This dualframework approach enabled a structured, theorydriven interpretation of findings while ensuring that barriers, facilitators, and implementation strategies were mapped in a consistent and comprehensive manner. The integration of both frameworks contributed to the conceptual clarity of the review and facilitated comparison between studies operating at different levels of implementation (innovation, professional, patient, organizational, and consumer-focused strategies).
The involvement of a multidisciplinary clinical academic research team in conducting this study, including occupational therapists, a nurse, a physiotherapist, a methodologist, and rehabilitation specialists, as well as a person with lived experience of multiple sclerosis, represents another significant strength. This diversity enriched the interpretative process and ensured that the findings were examined through multiple lenses. The iterative teambased review of search strategies, inclusion decisions, extractions, and interpretations enhanced the internal validity and practical relevance of the conclusions 34. Including a person with MS further grounded the work in enduser experience, ensuring that the synthesis reflected both clinical and realworld perspectives 35.
Despite its strength, this review also has some limitations. As is typical for mapping reviews, it did not include a formal critical appraisal of methodological quality. While mapping reviews are designed to provide an overview rather than evaluate study rigor, the absence of a quality assessment limits the ability to draw conclusions about the strength or reliability of the identified evidence. This means that while the review identifies which barriers, facilitators, and strategies are reported in the literature, it cannot determine how strongly these findings are supported by highquality empirical research.
Another limitation is that data selection was conducted by a single reviewer. Although this approach is not uncommon in mapping reviews, it introduces the possibility of bias in data-extraction and reduces reliability. Dual independent data-extraction could have increased methodological robustness.
Finally, the limited depth and variability of the evidence base itself. The included studies were heterogeneous in design—ranging from feasibility studies to qualitative research and small-scale trials—but often lacked detailed reporting on contextual factors or long-term sustainability.
Conclusion
Implementation of evidence-based occupational therapy for MS requires context-sensitive strategies across multiple levels, supported by practical tools like manuals, coaching, patient empowerment and sufficient organizational resources. However, limited attention to structural and financial barriers may compromise sustainability. Strengthening implementation through early planning, clear intervention descriptions, and collaboration among clinicians, researchers, and policymakers is essential to improve uptake and ultimately enhance patient outcomes and quality of life.
Knowledge translation takeaway
To facilitate the implementation of new evidence:
· Tailor mapped barriers, facilitators and implementation strategies to the specific setting.
· Develop and implement an action plan based on the mapped determinants.
· Identify and evaluate relevant quality indicators.
Use this mapping review as a supportive tool for implementing new evidence into OT for MS.
Disclosure
The authors used ChatGPT OpenAI to improve the language of the paper.
The authors have no conflicts of interest to declare for this study.
Supplementary Material
References
- 1.Grimshaw J M, Eccles M P, Lavis J N, Hill S J, Squires J E. (2012) Knowledge translation of research findings. Implement Sci. 7, 50-10.
- 2.Glasziou P, Straus S, Brownlee S, Trevena L, Dans L et al. (2017) Evidence for underuse of effective medical services around the world. , Lancet 390(10090), 169-177.
- 4.Graham I D, Logan J, Harrison M B, Straus S E, Tetroe J et al. (2006) Lost in knowledge translation: time for a map?. , J Contin Educ Health Prof 26(1), 13-24.
- 5.Negrini S, Arienti C, Armijo-Olivo S, Côté P, Heinemann A W et al. (2025) RCTRACK Executive Committee; GUIDE-Rehab Advisory Committee; Rehabilitation Journals Chief Editors; PREPARE Project Clinical Partners. Reporting guideline for intervention description in rehabilitation (GUIDE-Rehab): a tool to open the black box of rehabilitation complex interventions. , BMJ Evid Based Med doi:, 10-1136.
- 6.Field B, Booth A, Ilott I, Gerrish K. (2014) Using the Knowledge to Action Framework in practice: a citation analysis and systematic review. , Implement Sci 9, 172-10.
- 8.Kos D, Boers A, O'Meara C, Bekkering G E, L De Coninck et al. (2026) Occupational therapy for multiple sclerosis. Cochrane Database Syst Rev. 10-1002.
- 9.Kinney A R, Stearns-Yoder K A, Hoffberg A S, Middleton A, Weaver J A et al. (2023) Barriers and facilitators to the adoption of evidence-based interventions for adults within occupational and physical therapy practice settings: a systematic review. Arch Phys Med Rehabil. 104(7), 1132-1151.
- 10.Grol R, Grimshaw J. (2003) From best evidence to best practice: effective implementation of change in patients'. 362(9391), 1225-1230.
- 11.Mazza D, Bairstow P, Buchan H, Chakraborty S P, O Van Hecke et al. (2013) Refining a taxonomy for guideline implementation: results of an exercise in abstract classification. Implement Sci. 8, 32-10.
- 12.James K L, Randall N P, Haddaway N R. (2016) A methodology for systematic mapping in environmental sciences. Environ Evid. 5(1), 1-13.
- 13.Campbell F, Tricco A C, Munn Z, Pollock D, Saran A et al. (2023) Mapping reviews, scoping reviews, and evidence and gap maps (EGMs): the same but different—the Big Picture review family. Syst Rev. 12-1.
- 14.Grol R, Wensing M. (2004) What drives change? Barriers to and incentives for achieving evidence-based practice. , Med 180-6.
- 15.Plow M, Finlayson M. (2014) A qualitative study exploring the usability of Nintendo Wii Fit among persons with multiple sclerosis. Occup Ther Int. 21(1), 21-32.
- 16.Carandang K, Poole J, Connolly D. (2022) Fatigue and activity management education for individuals with systemic sclerosis: adaptation and feasibility study of an intervention for a rare disease. Musculoskelet Care. 20(3), 593-604.
- 17.Fakolade A, Finlayson M, Plow M. (2017) Using telerehabilitation to support people with multiple sclerosis: a qualitative analysis of interactions, processes, and issues across three interventions. Br J Occup Ther. 80(4), 259-268.
- 18.Barnett C, Murphy A, da Cruz DC. (2024) Acceptability and usability of assistive equipment and technology by individuals with multiple sclerosis: a qualitative study with occupational therapists. , Br J Occup Ther 87(11), 715-724.
- 19.Dwyer C P, Oglesby M H, Joyce R, Hynes S M. (2024) A cognitive occupation-based programme for people with MS: acceptability, feasibility, and experiences of people with multiple sclerosis. Disabil Rehabil. 46(14), 3026-3036.
- 20.Bowen M R, Augustyn J, Fisher L, Lawson L M. (2024) Feasibility of addressing the spiritual well-being of persons with multiple sclerosis: a mixed-methods program evaluation. , Am J Occup Ther 78(1), 7801205120-10.
- 21.Hynes S M, Forwell S. (2019) A cognitive occupation-based programme for people with multiple sclerosis: a new occupational therapy cognitive rehabilitation intervention. Hong Kong J Occup Ther. 32(1), 41-52.
- 22.Bove R M, Rush G, Zhao C, Rowles W, Garcha P et al. (2019) A videogame-based digital therapeutic to improve processing speed in people with multiple sclerosis: a feasibility study. Neurol Ther. 8(1), 135-145.
- 23.Kessler D, Franz M, Malakouti N, Rajachandrakumar R, Baharnoori M et al. (2024) Randomized controlled trial of occupational performance coaching for adults with multiple sclerosis. Arch Phys Med Rehabil. 105(9), 1649-1656.
- 24.B De Dios Perez, Holmes J, Elder T, Lindley R, Evangelou N et al. (2025) Implementing vocational rehabilitation for people with multiple sclerosis in the UK National Health Service: a mixed-methods feasibility study. Disabil Rehabil. 47(12), 3124-3136.
- 25.Afshar S, Akbarfahimi N, Ahmadi Kahjoogh M, Rassafiani M, Azimian M et al. (2024) Occupation-based intervention for people with multiple sclerosis: a feasibility study. , Int J MS Care 26(3), 254-258.
- 26.Askari S, Pappas C, C De Smit, Jackson E, King E et al. (2023) Comparison of goals set by people with multiple sclerosis during two fatigue management interventions. Scand J Occup Ther. 30(5), 684-692.
- 27.Simeon R, Galeoto G, Valente D, Conte A, Ferrazzano G et al. (2025) Fatigue management effects on social participation and environment management in individuals with multiple sclerosis: quasi-experimental study. Br J Occup Ther. 88(2), 93-104.
- 28.Comber L, Peterson E, O'Malley N, Galvin R, Finlayson M et al. (2021) Development of the Better Balance Program for people with multiple sclerosis: a complex fall-prevention intervention. , Int J MS Care 23(3), 119-127.
- 29.Cahill S, Richardson H. (2022) Shared decision making and reducing the use of low-value occupational therapy interventions. , Am J Occup Ther 76(3), 7603090010-10.
- 30.Varela A J, Gallamore M J, Hansen N R, Martin D C. (2025) Patient empowerment: a critical evaluation and prescription for a foundational definition. Front Psychol. 15, 1473345-10.
- 31.Alley Z M, Chapman J E, Schaper H, Saldana L. (2023) The relative value of pre-implementation stages for successful implementation of evidence-informed programs. Implement Sci. 18(1), 30-10.
- 32.Hoffman T C, Glasziou P P, Boutron I, Milne R, Perera R et al. (2014) Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. 348-1687.
- 33.Page M J, McKenzie J E, Bossuyt P M, Boutron I, Hoffmann T C et al. (2020) The PRISMA. , BMJ 2021, 372-71.